POLICY PAPER: “Morning-After” Abortion Pills Should be Opposed
The Morning-after Abortion Pill (MAP), which is commonly referred to by pro-abortion activists as a so-called “emergency contraception” drug, is actually a high dosage of hormones ordinarily found in physician-prescribed “birth control” pills. According to documentation from manufacturers of the MAP, the pill must be taken within 72 hours after sexual intercourse to be effective.(1) While the MAP’s primary purpose is to prevent ovulation, it is also designed to prevent the implantation of a fertilized egg when taken AFTER conception, thereby causing some chemical abortions.
3 REASONS FPN OPPOSES THE ‘MORNING-AFTER’ ABORTION PILL:
REASON 1: Because the MAP destroys tiny human lives
Even though the primary purpose of the MAP is to prevent conception by preventing ovulation, a secondary effect of the drug is to prevent an already-fertilized egg from attaching itself to the uterine wall. This secondary effect constitutes an abortion; it is the destruction of a tiny human life. Proponents often claim that such instances are rare. However, this claim is impossible to prove. Besides, even a handful of secondary-effect abortions occurring are unacceptable.
The general purpose of the MAP is to create a hormonal stimulation in the woman’s body that is similar to that of a natural pregnancy. The MAP operates in three possible ways:
-
- 1. It can delay or stop the release of an egg (ovulation).
-
- 2. It can prevent the sperm from fertilizing an egg by thickening the cervical mucous.
-
- 3.
It can decrease the thickness the uterine lining, preventing a fertilized egg (embryo) from implanting in the uterus
- (2)(3)
If the first two functions fail, then ovulation occurs and the egg becomes fertilized by the sperm, forming an embryo. However, the MAP slows the movement of the fertilized egg through the Fallopian tube. 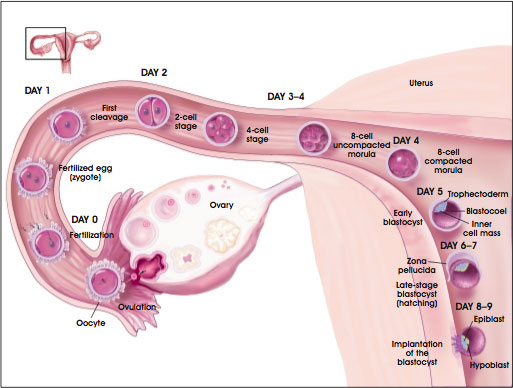 Meanwhile, the anti-implantation effect of the MAP will cause the endometrial wall to thin and shrivel, thereby making the uterus very hostile to the newly formed human life.(4) The end result is the inability of the embryo to implant in the uterus, resulting in the bodily rejection and expulsion of the new human life. One study showed this abortifacient effect of the pill is “probably the main mechanism of action of the morning after pill.”(5) According to researcher Dr. Walter Larimore, “endometrial thickness is related to the functional receptivity of the endometrium. [W]hen the endometrial lining becomes too thin, then implantation does not occur.”(6)
Meanwhile, the anti-implantation effect of the MAP will cause the endometrial wall to thin and shrivel, thereby making the uterus very hostile to the newly formed human life.(4) The end result is the inability of the embryo to implant in the uterus, resulting in the bodily rejection and expulsion of the new human life. One study showed this abortifacient effect of the pill is “probably the main mechanism of action of the morning after pill.”(5) According to researcher Dr. Walter Larimore, “endometrial thickness is related to the functional receptivity of the endometrium. [W]hen the endometrial lining becomes too thin, then implantation does not occur.”(6)
Although abortion activists argue that the MAP will not terminate a pregnancy already in progress, their definition of ‘pregnancy’ is a deliberate deception. The start of a pregnancy is defined as the union of an egg and a sperm (known as conception), resulting in the creation of a new human life. In every way, the union of these two elements marks the creation of a new human life. Therefore, the MAP does cause abortions to pregnancies already in progress.
In an obvious attempt to make the use of abortifacient drugs like the MAP more acceptable, abortion activists and pharmaceutical companies are waging a misinformation campaign to redefine the meaning of “pregnancy.” As a result, they have succeeded in convincing millions of the lie that a pregnancy begins at the point when the fertilized egg is implanted in the uterus, rather than the at the moment the sperm fertilizes the egg. Dr. Joseph Stanford, a professor at the University of Utah School of Medicine(7), calls this a “deliberate redefinition.”(8) Stanford, who was one of four dissenters on the FDA advisory board that approved the Plan B pill for over-the-counter distribution, argues that the pill does act as an abortifacient because of its post-fertilization effect on the uterus.(9)
One organization propagating the false definition of pregnancy is the American College of Obstetricians and Gynecologists (ACOG). According to the ACOG:
For a woman to become pregnant, a series of events must happen over a period of about a week and a half. All of the following events must occur:
1) She must ovulate.
2) Her egg must be fertilized by male sperm.
3) The fertilized egg
must implant itself
into the lining of her uterus.(10)
The sperm can reach a woman’s Fallopian tubes roughly 10 minutes after sexual intercourse is completed. Since the egg has a viability of about 24 hours, the sperm must travel up the Fallopian tubes to fertilize the egg within that period. However, since sperm are viable for a period of 3 to 7 days, pregnancy may occur if sexual intercourse occurs a few days before the release of the egg (ovulation).
Obviously, the MAP will only act to stop the release of the egg if it is taken before ovulation occurs. However, since the MAP is marketed to women who believe that they may have already ovulated, the MAP serves as an abortion drug far more often than the manufacturers will admit. The result of taking the MAP after ovulation is the hardening of the uterine wall so that the new zygote will be discharged from the uterus due to inability to implant. This is chemical abortion.
REASON 2: Because easy access to the MAP promotes promiscuity, yet the MAP offers no protection from STD’s
The ‘freedom from consequences’ that the MAP allows is a dangerous ‘freedom.’ Although the MAP does provide an ‘easy’ abortion for many women, it in no way prevents the user from contracting sexually transmitted diseases. The perceived lack of consequences will contribute to an even higher STD rate. A recent study in the United Kingdom found that “recent increases in the number of youth family planning clinic sessions had little overall impact on teenage pregnancy rates” and “led to significantly higher rates of diagnoses of STDs amongst teenagers.” The study also found that the “shift towards greater promotion of emergency birth control” has “worsened the impact on [STD] rates since 2000.”(11)
It seems as though abortion activists would like nothing more than to promote the MAP as a ‘contraceptive.’ Their success in convincing people that a pregnancy begins at implantation instead of conception leads to the removal of moral responsibility from women who, if they were aware of the MAP being an abortifacient, would refrain from using it.
The MAP does nothing to alleviate the root problem of promiscuity. Rather, by offering a so-called “easy” option to shirk the consequences of non-marital sex, this self-serve abortifacient only encourages people to become more sexually active with more partners. The rise in the acceptance of casual sex is evidenced by the name of the pill. “Morning-after” implies that aborting a baby is no big deal, like brushing one’s teeth or taking a shower. The MAP just adds one more item to the “morning-after” to-do list. With a misnomer like “emergency contraceptive pill,” its name draws attention away from parental responsibility, abstinence, and self-control; the only “emergency” that the MAP is named for is the ‘hassle’ of having a baby.
REASON 3: Because the MAP presents a dangerous health risk to women
High dosages of hormones interfere with the natural menstrual cycle and can often cause intense discomfort and pain. Common side effects for women who take the MAP are nausea, vomiting, breast tenderness, abnormal bleeding, headaches, and/or dizziness. (12) However, some women have also experienced more serious side effects that include severe abdominal pain, chest pain, shortness of breath, severe headaches, severe leg or arm pain, and/or eye problems. The MAP could also be a danger to women with existing medical problems such as a past heart attack or stroke, breast or genital cancers, liver cancer, and/or blood clots in the lungs or legs.(13)
Manufacturers have reduced the hormone content of oral contraceptives due to serious side effects and health risks. Now women are being encouraged to use these same pills, in multiple doses, as post-coital “contraception.” The potential long-term impact of these high hormone doses, especially when used repeatedly, is worrisome and not being adequately addressed. (14)
Abortion advocates falsely claim that the MAP is the safest drug of its kind on the market. However, there is a lack of scientific evidence regarding the safety of the MAP. (15) Since serious side effects don’t always immediately manifest themselves after taking pharmaceutical drugs, a high-dosage chemical drug like the MAP should not be used. In other words, just because women don’t immediately die after taking the MAP doesn’t validate the claim that the MAP is safe. It is not known whether the large amounts of chemicals in the MAP cause permanent damage to a woman’s fertility or cause certain diseases such as cancer to develop over time. Even though the MAP cannot abort a baby that has already been implanted in the uterus, the effect of the MAP’s dangerously large dosage of hormones on that baby are not yet known. The over-the-counter status of Plan B, a popular “emergency contraceptive” pill, communicates the false impression to women that the pill is safe to use, even on a regular basis, as if it were as harmless as cough medicine. The fact is, to date, there is no scientific study proving the maximum safe dosage for levornorgestrel, the active chemical in Plan B. (16)
Because there is a lack of data from scientific studies concerning the maximum safe dosage for this drug, as well as the unknown side effects resulting from long-term, repeated usage of the MAP, its use should be opposed. However, studies have linked long-term usage of other oral contraceptives containing smaller doses of chemicals with life-threatening conditions such as heart attack, certain cancers, and blood clots. (17) How much more dangerous is the high-dosage MAP?
CONCLUSION:
Human life begins at conception, which is the moment a sperm and egg unite to form an embryo. Since life begins at conception, it is wrong to purposefully prevent the continued existence of a baby at any stage of development. By design, the Morning-after Abortion Pill often executes a chemically-induced abortion by preventing embryos from implanting in the mother’s uterine wall. Therefore, the Morning-after Abortion Pill must be opposed as a matter of personal, corporate and public policy.
Beyond its abortifactient nature, there are health implications for women who take the MAP which alone merit opposing its use: the increased potential for the transmission of STD’s, the obvious consequences of such an intense and immediate hormone treatment, and the lack of controlled studies regarding the safety of the MAP’s long term use.
Endnotes:
1. http://www.go2planb.com/ForConsumers/TakingPlanB/Default.aspx
2. Carrie Gordon Earll, “Emergency Contraception (Morning After Pill)”, 2004, as found at http://www.family.org/cforum/fosi/bioethics/facts/a0030438.cfm
3. Physicians’ Desk Reference (Montvale, NJ: Medical Economics, 1998).
4. Abdalla HI, Brooks AA, Johnson MR, Kirkland A, Thomas A, Studd JW. “Endometrial Thickness: A Predictor Of Implantation In Ovum Recipients?” Human Reprod 1994;9:363-365. As found at http://www.epm.org/articles/bcp3300.html#_edn8.
5. Fabienne Grou, MD, Isabel Rodrigues, MD, M PH, “The morning-after pill – How long after?” Am. J. Obstet Gynecol. December, 1994, pp.1529-1534.
6. Walter L. Larimore and Joseph Stanford, “Postfertilization Effects of Oral Contraceptives and their Relation to Informed Consent.” Archives of Family Medicine 9 (February, 2000). As found at http://www.polycarp.org/larimore_stanford.htm.
7. http://uuhsc.utah.edu/dfpm/JStanford.htm
8. Elaine Jarvik, “U. doctor disputes claims for the ‘morning-after’ pill.” Deseret Morning News. October 3, 2006. As found at http://deseretnews.com/dn/view/0,1249,650195725,00.html
9. Walter L. Larimore and Joseph Stanford, “Postfertilization Effects of Oral Contraceptives and their Relation to Informed Consent.” Archives of Family Medicine 9 (February, 2000). As found at http://www.polycarp.org/larimore_stanford.htm.
10. American College of Obstetricians and Gynecologists Report. “A Closer Look at Emergency Contraception.” August 2001.
11. David Paton, “Random Behavior or Rational Choice? Family Planning, Teenage Pregnancy and STIs,” presented at the Royal Economic Society Conference, Swansea, April 2004. Cited with permission. www.swan.ac.uk/economics/res2004/program/papers/Paton.pdf
12. John Wilks, “A Consumer’s Guide to the Pill and Other Drugs”, 1997, as found at http://www.morningafterpill.org/mapinfo1.htm
13. Steven Mosher, “The Dangers of the Morning-After Pill”, PRI Weekly, 2004, as found at http://www.lifeissues.net/writers/mos/mos_15dangersmap.html
14. http://www.physiciansforlife.ca/html/life/abortion/articles/morningafterpill.html
15. Wendy Wright, “Talking Points on the Morning-After Pill (MAP)”, 2004, as found at http://www.cwfa.org/articles/5621/CWA/life/index.htm
16. “There are no data on overdosage of Plan B,” Plan B (Levonorgestrel) Emergency Contraception:
Prescribing Information, http://www.go2planb.com/section/prescribing_info/?PHPSESSID=50065b3c473d1c2d512226d7230b5596. As found at www.cwfa.org/images/content/mapalec.pdf
17. Helen C. Pymar, Mitchell D. Creinin, “The Risks of Oral Contraceptives,” Seminars in Reproductive Medicine, 19 (4): 305-312, 2001
Prepared by FPN Policy Analyst Alexander Mason. Copyright, 2006 to 2010. All Rights Reserved.